This 2016 paper reviews evidence suggesting metformin may counteract the beneficial effects of exercise in diabetics. Metformin is the most widely used prescription drug to treat hyperglycemia in Type 2 diabetics and is recommended as a first-line treatment by the American Diabetes Association (1). The authors note metformin is also increasingly prescribed for CVD and cancer risk reduction, even among nondiabetic Americans (2).
Both exercise and metformin have been shown to independently improve glycemic control and insulin sensitivity in diabetics; the former has also been shown to drive cardiovascular improvements. Multiple studies have shown, however, that the combination of metformin and exercise leads to an inferior response compared to either intervention alone. For example:
- One study showed metformin alone and exercise alone led to 55% and 90% improvements in skeletal muscle insulin sensitivity, respectively. Significantly, however, metformin + exercise led to a smaller improvement at 30% (3).
- Metformin combined with exercise led to smaller improvements in both hsCRP and systolic blood pressure — and thus a smaller reduction in cardiovascular risk — than either intervention alone. (ibid)
- Adding metformin to exercise blunted subjects’ increase in VO2max by 50% compared to 10 weeks of exercise alone. Subjects also reported greater perceived exertion than controls while exercising and taking metformin, which further indicates a reduction in cardiovascular improvement. These reduced improvements in aerobic fitness were associated with blunted improvements in muscular insulin sensitivity (4).
- Similar effects have been seen with statins, where aerobic exercise training alone in overweight/obese adults improved VO2max by 10%, but when combined with statins therapy, VO2max improved by only 1.5% (5).
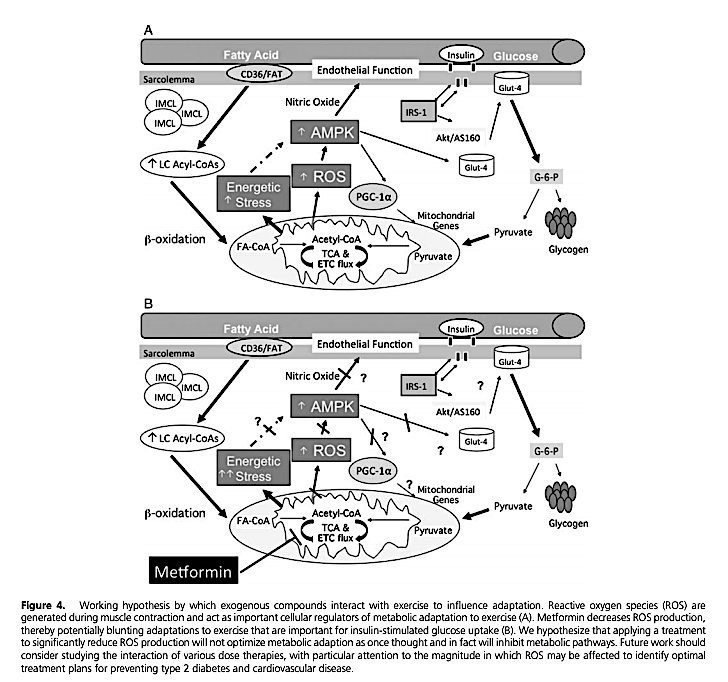
Figure 4 summarizes the authors’ proposed mechanism to explain these observations. Exercise — specifically muscular contraction — leads to the production of reactive oxygen species (ROS). This ROS increase leads to greater AMPK activation, which then increases muscular endothelial function (by increasing the effects of nitric oxide) and glucose uptake (by increasing translocation of Glut-4 transporters to the surface of muscle cells). Metformin inhibits production of ROS and thus undermines the primary mechanism by which muscle cells increase aerobic and metabolic function in response to exercise.
The authors comment that metformin alone has been shown to have beneficial effects in diabetic subjects, and thus, its use as a treatment should not be categorically discouraged. However, in exercising overweight, obese, and/or diabetic subjects, metformin (and possibly statins) may counteract the beneficial effects of exercise. It therefore may not be advisable as a first-line therapy for these populations.
References
-
American Diabetes Association. Pharmacologic approaches to glycemic treatment: Standards of medical care in diabetes—2019. Diabetes Care 42.1(Jan. 2019): S90-S102. Available here.
-
Rhee, MK, et al. Many Americans have pre-diabetes and should be considered for metformin therapy. Diabetes Care 33.1(Jan. 2010): 49-54. Available here.
-
Malin, SK, et al. Independent and combined effects of exercise training and metformin on insulin sensitivity in individuals with prediabetes. Diabetes Care 35.1(Jan. 2012): 131-6. Available here.
-
Malin, SK, et al. Metformin’s effect on exercise and postexercise substrate oxidation. Int J Sport Nutr Exerc Metab. 20.1(Feb. 2010): 63-71. Available here.
-
Mikus CR, et al. Simvastatin impairs exercise training adaptations. J Am Coll Cardiol. 62.8(Aug. 2013): 709-14. Available here.
Impact of Metformin on Exercise-induced metabolic adaptations to lower type 2 diabetes risk