This article discusses the diet-heart hypothesis, the main reasons why it became dominant, and how it has led to dietary guidelines that have driven an unprecedented change in eating habits in most of the developed world. Future articles will look at the weaknesses in the hypothesis from physiological, epidemiological, and interventional perspectives.
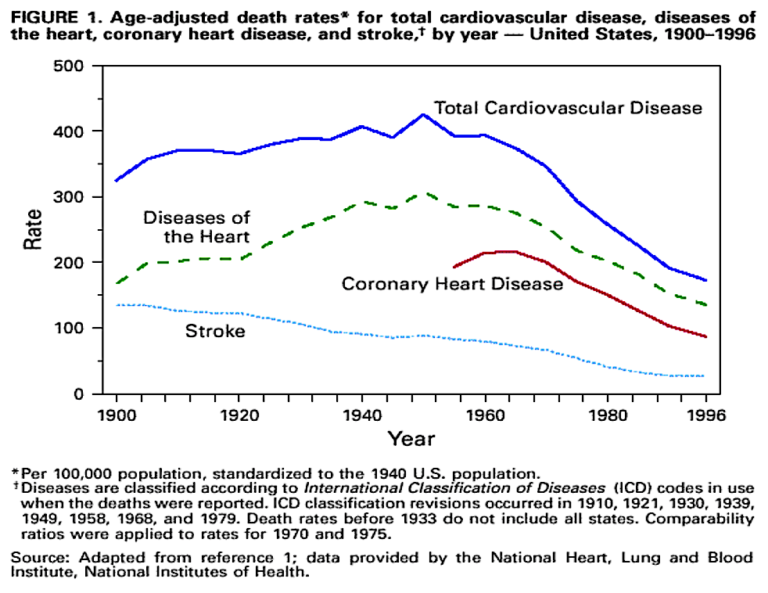
It is generally accepted that cardiovascular disease, primarily coronary heart disease (CHD), first appeared as a modern “epidemic” in the U.S. shortly after the Second World War. As the U.S. did not begin using the International Classification of Diseases (ICD) system until 1948, a diagnosis of CHD could not be made before this time, so the exact rate of CHD prior to 1948 can only be, to a degree, guesswork.
However, it is probably true that CHD (however labeled) was very rare before the First World War, then steadily rose in prevalence during the 1920s, ‘30s, and ‘40s. By the 1950s, the death rate from CHD had reached a point whereby, within a 10-year period, one in 10 men was dying from a myocardial infarction. The mortality rate for women was about one-quarter that of men, although this differential was narrower in older age groups. The current rate in the U.S. is about one-fifth of this peak level.
In the 1940s and 1950s, there was little agreement about what had led to this “sudden” explosion of cardiovascular disease, although there had been speculation about dietary causes for many years.
What was known was that atherosclerotic plaques (thickening and narrowing of arteries), which are the underlying problem in all forms of CVD, contained “fat(s)” and cholesterol. It seemed probable that this fat and cholesterol had been deposited from the bloodstream.
A brief history of early knowledge about cholesterol
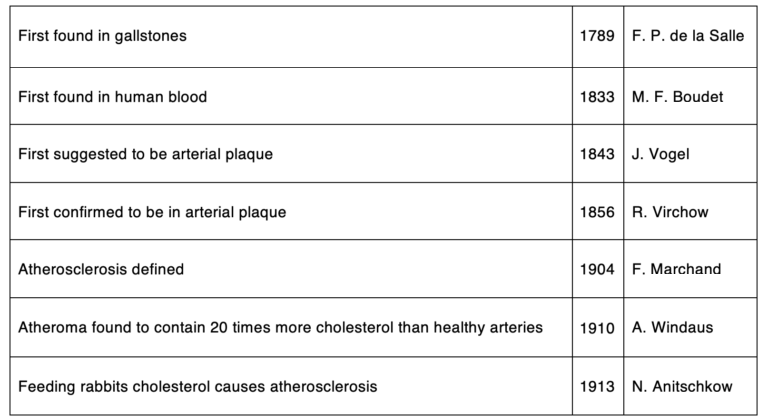
The information about cholesterol was purely of academic interest for many years. However, when CVD emerged as the leading cause of morbidity and mortality in the Western world, interest in cholesterol sharpened.
One researcher, Ancel Keys, who became the leading proponent of the diet-heart hypothesis, believed that cholesterol in the diet was likely the cause of raised cholesterol levels in the blood. The excess cholesterol was then deposited in the artery wall, leading to atherosclerotic plaques (thickenings and narrowings within the artery wall). This was the simplest version of the diet-heart hypothesis.
Keys then carried out a great deal of further epidemiological research, and he also performed a number of cholesterol feeding experiments in humans. He was surprised to find that, in humans, cholesterol had little or no effect on blood cholesterol levels or risk of atherosclerosis. He wrote:
The evidence — both from experiments and from field surveys — indicates that cholesterol content, per se, of all natural diets has no significant effect on either the cholesterol level or the development of atherosclerosis in man. (1)
Keys then shifted sideways from cholesterol to saturated fat in the diet, leading to the creation of the highly influential “Keys equation,” which he claimed could predict the effect of saturated and polyunsaturated fatty acids in the diet on serum cholesterol levels. (This equation uses the SI units of mmol/L, which is not used in the U.S., but the basic equation is the same.)
Cholesterol (mmol/L) = 0.031(2Dsf − Dpuf) + 1.5√Dch
Where Dsf is the change in percentage of dietary energy from saturated fats, Dpuf is the change in percentage of dietary energy from polyunsaturated fats, and Dch is the change in intake of dietary cholesterol. (Strangely, cholesterol remained in this equation despite Keys’ earlier research demonstrating that dietary cholesterol had no impact on the cholesterol level.)
In 1961, Keys stated, “No other variable in the mode of life besides the fat calories in the diet is known which shows such constant relationship to the mortality rate from coronary or degenerative heart disease.” He appeared on the cover of Time magazine as “Mr. Cholesterol.”
Despite a growing acceptance of this “somewhat altered” diet-heart hypothesis, no explanation was given as to how saturated fat raised blood cholesterol levels or how raised blood cholesterol levels causes atherosclerosis to develop. It was simply believed that A caused B and B caused C.
The lack of any obvious mechanism of action did not prevent the diet-heart hypothesis from coming to dominate thinking about CVD.
It can often take decades for an idea to move from scientific acceptance to public and political recognition. However, by 1977, articles published in the lay press were including things like this:
Photos taken inside clogged city sewer pipes look nearly identical to medical photos of the blood vessels of patients who have spent a lifetime gorging on fried chicken, sausage and bacon. “It’s like your arteries,” said John Parker, environmental compliance inspector with the city’s Water and Sewer dept. “Grease builds up in there. It’s gory.” (Savannah Morning News)
It was also in 1977 that the U.S. Senate Select Committee on Nutrition and Human Needs, set up by Senator George McGovern in 1968, announced the publication of its guidelines. They contained six main goals:
Goal 1. Increase carbohydrate consumption to account for approximately 55 to 60 percent of energy (caloric) intake.
Goal 2. Reduce overall fat consumption from approximately 40 percent to 30 percent of energy intake.
Goal 3. Reduce saturated fat consumption to account for about 10 percent of total energy intake; and balance that with polyunsaturated and monounsaturated fats, which should account for about 10 percent of energy intake.
Goal 4. Reduce cholesterol consumption to about 300 mg a day.
Goal 5. Reduce sugar consumption by about 40 percent to account for about 15 percent of total energy intake.
Goal 6. Reduce salt consumption by about 50 to 85 percent to about 3 g/day.
This became the basis for all the nutritional and dietary advice then followed, including the U.K.’s eatwell plate, the food pyramid in the U.S., and suchlike. The guidelines remain essentially unchanged today. The U.K. launched separate guidelines in 1983, but they were very much a carbon copy of the McGovern documents.
Shortly after this, in 1982, there was a National Cholesterol Consensus Conference. The primary conclusion was as follows:
It has been established beyond a reasonable doubt that lowering definitely elevated blood cholesterol levels (specifically, blood levels of Low-Density Lipoprotein [LDL] Cholesterol will reduce the risk of heart attacks caused by coronary heart disease.
The definition of high cholesterol was also lowered from 280 mg/dL (7.2 mmol/L) to 200 mg/dL (5.2 mmol/L). There were some dissenting voices, but most of the world had now swung behind both parts of the diet-heart hypothesis.
 Malcolm Kendrick is a family practitioner working near Manchester in England. He has a special interest in cardiovascular disease, what causes it, and what may prevent it. He has written three books: The Great Cholesterol Con, Doctoring Data, and A Statin Nation. He has authored several papers in this area and lectures on the subject around the world. He also has a blog, drmalcolmkendrick.org, which stimulates lively debate on a number of different areas of medicine, mainly heart disease.
Malcolm Kendrick is a family practitioner working near Manchester in England. He has a special interest in cardiovascular disease, what causes it, and what may prevent it. He has written three books: The Great Cholesterol Con, Doctoring Data, and A Statin Nation. He has authored several papers in this area and lectures on the subject around the world. He also has a blog, drmalcolmkendrick.org, which stimulates lively debate on a number of different areas of medicine, mainly heart disease.
He is a member of THINCS (The International Network of Cholesterol Sceptics), which is a network of doctors and scientists who believe that cholesterol is not the main underlying cause of heart disease. He remains a proud Scotsman, whisky drinker, and failed fitness fanatic who loves a good scientific debate — in the bar.
REFERENCES
- Keys A and Anderson JT. The relationship of the diet to the development of atherosclerosis in man. National Research Council DoMS. Ed. Symposium on atherosclerosis. Washington: National Academy of Sciences – National Research Council, 1954: 181-96.
Comments on The Diet-Heart Hypothesis, Part 1
The primary tragedy of the diet-heart hypothesis may not be its genesis, but its durability. As Kendrick noted, the link between fats and heart disease was not entirely without basis - Keys had observed associations. But it was without a compelling mechanism to explain WHY eating fat caused heart disease, beyond the intuitively appealing but scientifically unsupported claims like the "clogged sewer pipes" analogy.
If the Diet-Heart Hypothesis had been recognized for what it was - a single hypothesis on the origin and cause of heart disease, which deserves to be tested on an even playing field against other hypotheses backed by similar levels of evidence - it might have helped accelerate our understanding of heart disease by stimulating a vigorous scientific debate. Of course, most of us here know this is the opposite of what happened.
Clarke Read's suggestion that the missing key was simply a "compelling mechanism to explain WHY eating fat caused heart disease" presupposes that fat is indeed causing atherogenesis. Dr. Kendrick's and others' work is very clearly pointing elsewhere. Like all hypotheses, the diet-heart hypothesis deserved to be tested—it was. Other than making the pharmaceutical industry wealthy, it has failed, yet its shadow continues causing untold suffering to millions.
The Diet-Heart Hypothesis, Part 1
2