One of the characteristics of the modern Western diet is a massive imbalance in the ratio of omega-6 fats (n6) to omega-3 fats (n3) (i.e., the n6/n3 ratio). This change has been driven primarily by an enormous increase in n6 fat intake over the past 40 years, while the amount of n3 fats in the diet has remained stable or even decreased a little. The typical n6/n3 ratio in Westernized countries is ~15:1 (if not higher), whereas that in pre-industrial-seed-oil times was closer to ~4:1 (if not lower).
Concurrent with this enormous distortion of the n6/n3 ratio has been an increased prevalence of nonalcoholic fatty liver disease (NAFLD) in adults and even children. Medical authorities have posited multiple causes for this troubling increase in NAFLD, which could be considered to have reached epidemic proportions, since estimates suggest approximately a quarter to a third of adults are affected. The condition is now common even in adolescents.
The authors of this 2019 study hypothesized the increase in the n6/n3 ratio causes deposition of fat in the liver, and decreasing the fatty acid ratio to the lower levels that were common decades ago might promote the shedding of liver fat. Toward that end, they designed the experiment to determine what, if any, reduction in liver fat would occur solely from a change in diet that achieved a large decrease in the n6/n3 ratio while maintaining a weight-stable caloric intake.
In this single-arm trial, investigators recruited 20 obese adolescents, all of whom had fatty livers, into the study. They chose adolescents, because NAFLD is a growing problem in this demographic, and adolescents are notorious for consuming copious amounts of junk foods typically composed of a combination of wheat and/or corn, sugar, and vegetable oils with a high n6/n3 ratio.
The subjects then were prescribed a diet equal in calories to their starting diets but with a much lower n6/n3 ratio; they consumed only foods provided by the investigators. Calories were adjusted throughout the 12-week duration of the study to ensure the subjects were adhering to intake levels sufficient to maintain their starting weight, obviating weight loss as an attributable cause for any changes observed.
Abdominal MRI and oral glucose tolerance testing were performed at the start and again at the end of the 12-week trial. During the trial, investigators monitored OXLAMs (oxidized derivatives of linoleic acid, the primary unsaturated fat in vegetable and seed oils) to ensure compliance.
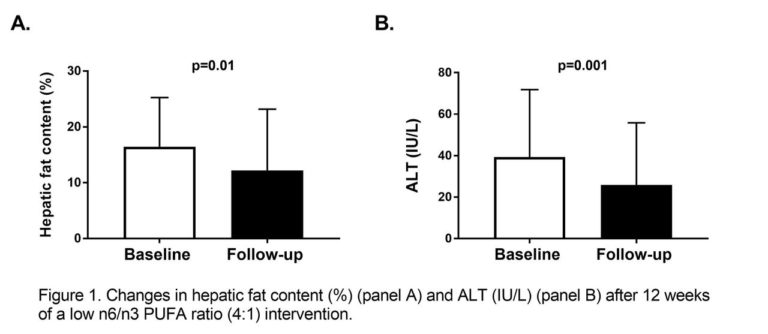
By the end of the study, among the 17 subjects who had completed the trial, liver fat had decreased by 26 percent. Also, ALT concentrations (an enzymatic measure of liver health), triglycerides, cholesterol, and insulin resistance had all improved by a significant amount.
The results imply that a simple reduction of the n6/n3 ratio, even without a caloric reduction, will reduce fatty liver in adolescents in the absence of weight loss.