Chronic kidney disease of unknown origin (CKDu) is responsible for the deaths of at least 20,000 Nicaraguan sugarcane workers and afflicts thousands of laborers in Brazil, El Salvador, Egypt, India, Qatar, and Sri Lanka, as well. And this disease is spreading to the U.S.—as Bloomberg published last year, “hospitals in the U.S. are reporting a sharp increase in patients whose symptoms are consistent with the disease.” In one study, one-third of participating Florida agricultural workers suffered from acute kidney injury.
From Nicaragua to Miami, cases of chronic kidney disease of unknown origin (CKDu) share a common setting: sites where agricultural work takes place in severe heat. Independent research on the cause of CKDu points to chemicals used in sugarcane agriculture, the physiological response to intensive work in the heat, and the sugary beverages commonly consumed by laborers. But researchers receiving millions in funds from the Centers for Disease Control and Prevention, the National Institutes of Health, and the Central American sugar industry have failed to discover the disease’s cause—or investigate some of the leading suspects.
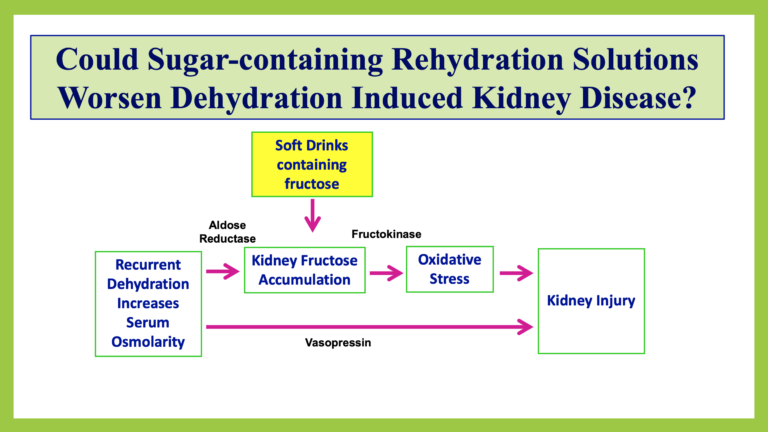
Research directed by nephrologist Dr. Richard Johnson of the University of Colorado suggests that a combination of heat stress, dehydration, and sugar-sweetened beverages is toxic to the kidneys.
From “Mesoamerican Nephropathy: A CKD of unknown etiology in Central America,” a presentation by Carlos A. Roncal-Jiménez, University of Colorado
Dr. Johnson’s University of Colorado Anschutz colleague Miguel Lanaspa Garcia also notes that Central American sugar workers “don’t trust water … . They think water makes them sick,” which leaves workers with few options besides sugar-sweetened beverages. Johnson concludes, “the most important reasons [for rising rates of CKD] are increasing heat extremes (heat waves) coupled with hydration with sugary or, less commonly, alcoholic beverages.”
New research, such as “Soft Drink Consumption During and Following Exercise in the Heat Elevates Biomarkers of Acute Kidney Injury,” has been consistent with Dr. Johnson’s theory. And the new evidence from human subjects is significant because much of Johnson’s work heretofore has focused on animal rather than human testing. (Also significant: Mountain Dew, the beverage used in this study, is produced by PepsiCo, a company that has explicitly marketed hyper-consumption of its sugar-sweetened beverages to people exercising for extended periods of time in the heat.)
The U.S. CDC is the government agency responsible for preventing the spread of epidemics in the United States. In fact, the CDC has been investigating the CKDu problem since at least 2014. Why, then, does this epidemic’s origin remain unknown, even as it has started affecting Americans?
One potential answer lies within the CDC’s partnership with the sugar industry to lead the CKDu investigation. Instead of going through an open bidding process, Boston University researchers with a history of sugar industry funding “approached the CDC with a proposal, and funding was then obtained from the sugar industry.” In 2014, the Central American sugar industry funneled $1.7 million through the CDC’s own foundation. Contrary to federal law, the CDC Foundation’s 2014 annual report failed to list the restrictions or amount of one industry gift (“Los Azucareros del Istmo Centroamericano”) and completely omitted a $675,000 payment from the National Committee of Sugar Producers of Nicaragua—the 2015 report did list a payment from NCSPN but did not include its amount or restrictions, despite federal law requiring the foundation to disclose this information.
This pattern of inconclusive “research” is similar to the industry-funded alcohol study canceled by the National Institutes of Health after industry-researcher communications came to light and the NIH accused its own officials of “steering funding to a pre-selected investigator.”
Yet the sugar industry’s ongoing sponsorship of this research stands out even among the many NIH and CDC partnerships with corporations that represent conflicts of interest. The sugar industry has a strong incentive to downplay at least three of the suspected causes of CKDu. Can one imagine the sugar industry acknowledging that sugar-sweetened beverages are a cause of CKDu? Or blaming illness on the herbicides used by industry laborers (glyphosate, to be specific)? And what of the intense working conditions the industry imposes on its workers?
Research clearly implicating any one of those factors could imply massive corporate liability resulting from culpability in the deaths of thousands of laborers around the world. On the other hand, ambiguous research that called for further study would prevent any such corporate liability, even as it ensured the continued flow of research funding to the so-called guardians of public health.